- Skin lesions
- Itching
- Dry skin



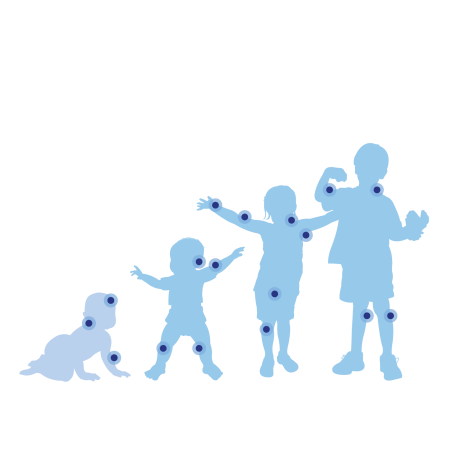
The lesions of atopic eczema are found on characteristic areas of the body, which evolve with age5
- In infants: the main areas affected are the face (forehead, cheeks, chin) and the outer surface of the arms and thighs.
- In children: they are mainly found on the elbow and wrist folds and on the back of the knees.
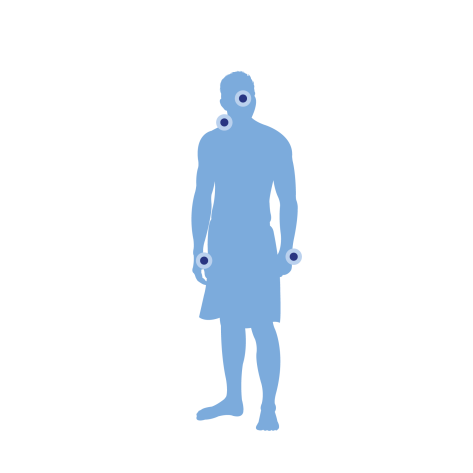
- In adults, if atopic dermatitis persists, it is often the neck and face alone that are affected by eczema. Sometimes the affected area can be generalised but more pronounced on the elbow and knee creases. The hands are also frequently affected and the symptoms can be aggravated by work.
- Contact eczema
- Varicose eczema
- Nummular eczema



Simple measures can improve the effectiveness of treatments
Regularly cut fingernails


Our hygiene recommendations for skin with an atopic tendency
Avoid hot showers or baths as this intensifies itching
Dab to dry
Use appropriate toiletries


Some tips to limit atopic eczema flare-ups
Opt for showers
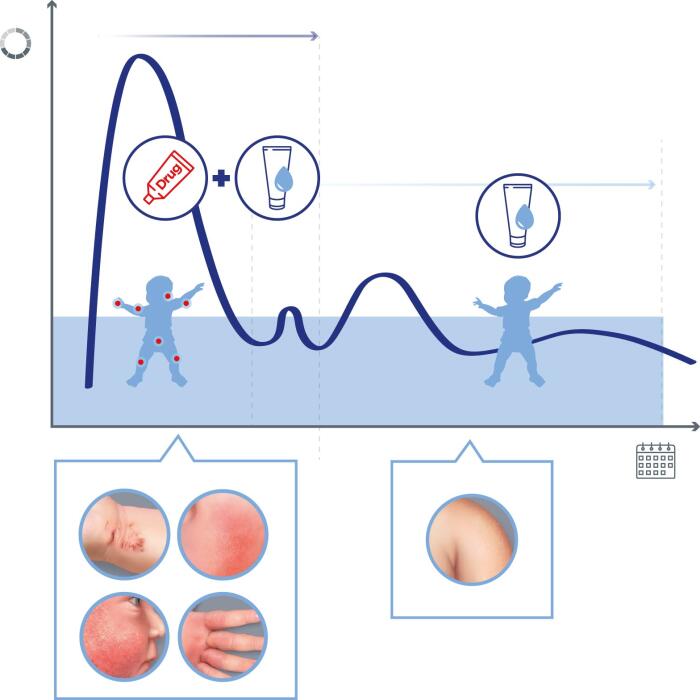
Apply an emollient
Apply the emollient once or twice a day



DEXERYL Emollient Cream: the skin partner for dry and sensitive skin
The basis for treating xerosis is, above all, moisturising the skin and appropriate hygiene.
DEXERYL supports you with emollient skin care and cleansers specially formulated for sensitive skin and recommended for the treatment of signs of skin dryness (xerosis).
DEXERYL Emollient Cream
DEXERYL Emollient Cream can be used to protect the skin and treat the signs and symptoms of dry skin, particularly in the context of atopic dermatitis, thanks to:
- glycerol for its hydrating action
- vaseline and paraffin for their protective role











What is eczema?
Managing eczema in babies
Managing eczema in adults?
The Different Types of Eczema: How to Recognise Them?
Causes of Eczema: Why Does It Occur and How Can You Prevent It?
Eczema treatments
Eczema Symptoms: Identification and Understanding






